From Prediction to Practice: A Task-Aware Evaluation Framework for Blood Glucose Forecasting
arXiv cs.LG / 5/4/2026
📰 NewsDeveloper Stack & InfrastructureSignals & Early TrendsModels & Research
Key Points
- The paper argues that standard aggregate metrics for clinical time-series forecasting can hide dangerous failures in high-risk regimes, motivating task-aware evaluation for blood glucose forecasting.
- It introduces two evaluation arms tailored to downstream uses: hypoglycemia early warning measured with event-level recall and patient-day false alarms, and insulin dosing decision support that tests action-dependent effects.
- Using real data from three clinical cohorts, the study finds models with high overall recall (above 0.9) can still perform poorly in the post-bolus period, where missed warnings have the greatest clinical consequences.
- For insulin dosing support, the framework uses the FDA-accepted UVA/Padova simulator to run paired factual/counterfactual scenarios, showing that strong real-data forecasters may fail to predict intervention effects and may recommend poor insulin doses under a clinically motivated cost function.
- The authors release a benchmark, a standardized preprocessing pipeline, and an interventional simulator-based dataset to enable reproducible, task-relevant model evaluation.
💡 Insights using this article
This article is featured in our daily AI news digest — key takeaways and action items at a glance.
Related Articles
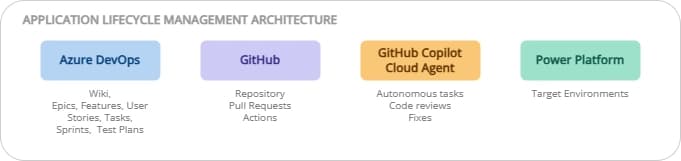
ALM on Power Platform: ADO + GitHub, the best of both worlds
Dev.to

Iron Will, Iron Problems: Kiwi-chan's Mining Misadventures! 🥝⛏️
Dev.to
Experiment: Does repeated usage influence ChatGPT 5.4 outputs in a RAG-like setup?
Dev.to
Open source models are going to be the future on Cursor, OpenCode etc.
Reddit r/LocalLLaMA
How I Automated VPN Deployment with AI: The World's First AI-Powered VPN Kit
Dev.to