CSRA: Controlled Spectral Residual Augmentation for Robust Sepsis Prediction
arXiv cs.LG / 4/17/2026
📰 NewsModels & Research
Key Points
- The study introduces CSRA (Controlled Spectral Residual Augmentation) to improve short-window sepsis prediction from multi-system ICU time-series data where limited history and scarce future supervision make learning difficult.
- CSRA groups clinical variables by system, learns system-level and global representations, and generates input-adaptive, spectrally controlled residual perturbations that produce structured and clinically plausible trajectory variants.
- The method is trained end-to-end with downstream predictors using a unified objective that includes anchor consistency loss and controller regularization to enhance augmentation stability and controllability.
- On MIMIC-IV sepsis data across multiple downstream models, CSRA improves prediction accuracy, cutting regression error by 10.2% in MSE and 3.7% in MAE versus a no-augmentation baseline, with consistent gains for classification as well.
- CSRA shows stronger robustness to clinical constraints by retaining benefits with shorter observation windows, longer horizons, and smaller training datasets, and it also generalizes to an external dataset (ZiGongICUinfection).
Related Articles
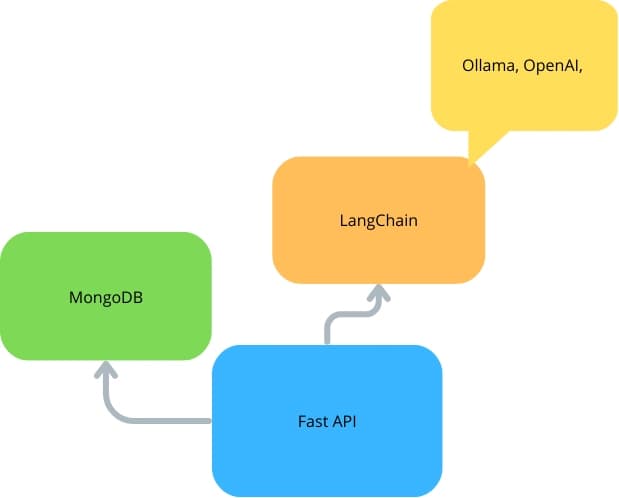
FastAPI With LangChain and MongoDB
Dev.to
![[2026] OpenTelemetry for LLM Observability — Self-Hosted Setup](/_next/image?url=https%3A%2F%2Fmedia2.dev.to%2Fdynamic%2Fimage%2Fwidth%3D1200%2Cheight%3D627%2Cfit%3Dcover%2Cgravity%3Dauto%2Cformat%3Dauto%2Fhttps%253A%252F%252Fdev-to-uploads.s3.amazonaws.com%252Fuploads%252Farticles%252Flu4b6ttuhur71z5gemm0.png&w=3840&q=75)
[2026] OpenTelemetry for LLM Observability — Self-Hosted Setup
Dev.to
The AI Education Product on Product Hunt Worth Watching
Dev.to

The joy and pain of training an LLM from scratch
Reddit r/LocalLLaMA

Did you know that you can use Qwen3.5-35B-A3B-Base as an instruction/reasoning Model?
Reddit r/LocalLLaMA